Abstract and Introduction
Abstract
We performed a systematic review of controlled trials on anxiety disorders treatment (generalized anxiety disorder, panic disorder, social phobia and post-traumatic stress disorder) published from 1980 to 2006, and identified trials comparing the efficacy of benzodiazepines (BZD) with that of antidepressants, in particular comparisons between BZD and newer antidepressants. Among 969 publications, 274 double-blind randomized controlled studies remained after using our exclusion criteria. These studies comprised altogether 439 comparisons. There were in total 23 comparisons of antidepressants versus BZD. Among these, 22 compared the efficacy of older antidepressants versus BZD, whereas only 1 concerned the comparison of a newer antidepressant versus BZD. It showed comparable efficacy between venlafaxine and diazepam in the treatment of generalized anxiety disorder. Our study shows that the major change of prescribing pattern from BZD to newer antidepressants in anxiety disorders has occurred in absence of comparative data of high level of proof.
Introduction
In the last decade, there was an important shift of prescribing pattern from BZD to newer antidepressants, with an almost 3-fold increase of the prescriptions of the latter. This increase exceeds that for depression diagnosis.[1,2]
There was also a shift in the expert opinions; in two surveys among experts in anxiety disorders, a clear change of preferences was noted, from BZD in 1992 to newer antidepressants in 1997.[3] In evidence-based medicine, when two or more options of treatment are available, the decision-making process should ideally be based on direct comparison of efficacy and side-effects.We examined a sample of expert opinions and psychiatric guidelines. In the treatment of anxiety disorders, both BZD and antidepressants were recognized as efficacious and the risk of dependence to BZD was evoked. However, neither experts nor guideline panels mentioned trials with direct comparisons (of efficacy or side-effects) between BZD and newer antidepressants.[3,5,6]
Hence, we formulated the hypothesis that the major change of prescribing pattern may have occurred in absence of adequate comparative evidence of efficacy, i.e., randomized controlled trials with direct comparison between newer antidepressants and BZD in anxiety disorders. The objective of this study was to assess if this comparative evidence indeed exists
Method
We performed a systematic review of the literature on the pharmacotherapy of anxiety disorders, using a reproducible Medline search syntax (available from the authors). Studies on the pharmacotherapy of anxiety disorders, comprising at least one arm with benzodiazepines or antidepressants, were included. Tricyclic/tetracyclic antidepressants and monoamine oxidase inhibitors were grouped under the label of older antidepressants. SSRIs and other recent antidepressants were grouped under the label of newer antidepressants (Table 1).
We set limits to publication dates from 1980 to 2006, to randomized controlled trials, and human trials. Studies with the following characteristics were excluded manually after the Medline search: methodology other than double-blind randomized controlled trial; non-pharmacological comparators (e.g., cognitive behavioral therapy) as well as trials with neither BZD, nor antidepressants in monotherapy as an arm (e.g., discontinuation and augmentation studies); redundant data (e.g., duplicate publications, analyze of subgroups); provoked panic attacks in experimental conditions (e.g., lactate, carbon dioxide); language of publication other than English; and diagnosis other than panic disorder, generalized anxiety disorder, social phobia and post-traumatic stress disorder (e.g., obsessive-compulsive disorder, depression with anxious symptoms, other specific phobia, anxious syndrome unspecified). Obsessive-compulsive disorder is not recognized as an indication for primary treatment using a BZD and was therefore not included in our study. Studies with several clinical entities were classified according to the diagnosis of the greater number of patients. The vast majority of excluded studies did not meet diagnosis criteria; many of them met two or more exclusion criteria.
We listed the trials comparing the efficacy of BZD with antidepressants, in particular those concerning newer antidepressants. We also listed the comparisons between antidepressants and placebo, BZD and placebo, antidepressants and antidepressants, BZD and BZD, and antidepressants/BZD and another compound.
We listed comparisons rather than only trials, since a given trial may comprise several comparisons.
Results
We identified 969 publications, when the search syntax was performed in January, 2007. After exclusions, 274 double-blind randomized controlled studies remained (the complete list of references for the trials selected can be obtained from the first author). These studies comprised altogether 439 comparisons. Panic disorder was the entity with the highest number of trials, i.e., 110 double-blind randomized comparative trials containing 170 comparisons, during a 27-year period. Generalized anxiety disorder was next, with 87 trials containing 174 comparisons.
There were in total 23 comparisons of antidepressants versus BZD. Among these, 22 compared the efficacy of older antidepressants versus BZD (Figure 1), whereas only 1 concerned the comparison of a newer antidepressant versus BZD.[7] It showed comparable efficacy between venlafaxine and diazepam.
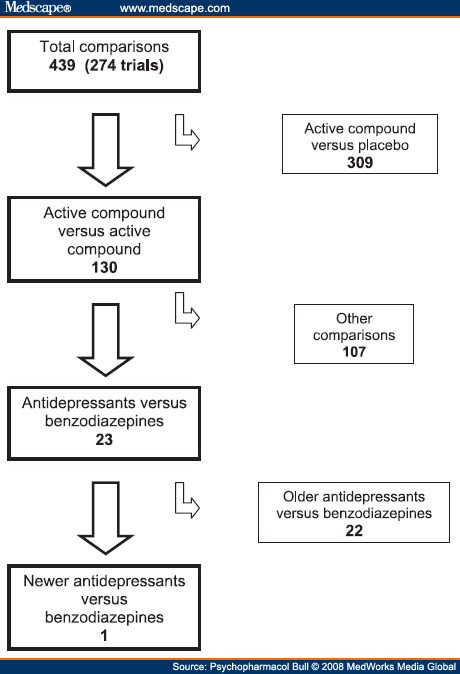 |
Figure 1. (click image to zoom) Number of double-blind comparisons in randomized controlled trials on pharmacological treatment of anxiety disorders.
|
We also found 183 comparisons between antidepressants and placebo (113 concerning newer antidepressants) and 90 comparisons between BZD and placebo. Also, 86 comparisons concerned an antidepressant or a BZD versus other compounds, or other compounds versus placebo. There were a total of 309 comparisons where the comparative compound was placebo, i.e., more than 70%. Antidepressants were compared to antidepressants 37 times and BZD were compared to BZD 20 times. Table 2 gives the overview as to the number of comparisons for each anxiety disorder and for each category of comparisons
Discussion
Our study clearly shows that the change of prescribing pattern from BZD to newer antidepressants was not based on evidence of a high level of proof, since there is only one double-blind, randomized controlled trial comparing one of these antidepressants to a BZD, among 274 double-blind, randomized controlled trials on drug efficacy in panic disorder, generalized anxiety, social phobia and post-traumatic stress disorder. This single study is that of Hacket and collaborators, about the efficacy of venlafaxine XR and diazepam in generalized anxiety disorder.[7] No statistically significative difference was found between these two compounds. In other words, a major change of prescribing pattern from BZD to newer antidepressants has occurred all around the world in the absence of comparative studies with a high level of proof. Such a situation is surprising, considering that the declaration of Helsinki insists on the fact that, if a comparative compound is available, it should be used in clinical trials of new molecules. It is stated in the article 29 of the Declaration of Helsinki that "the benefits, risks, burdens and effectiveness of a new method should be tested against those of the best current prophylactic, diagnostic and therapeutic methods."[8] Various reasons, not mutually exclusive, could explain this change of prescribing pattern.
Efficacy
The change from BZD to newer antidepressants may have been in the interest of the patients, but this remains to be proven with studies of high level of proof. Nevertheless, the change from BZD to newer antidepressants could be explained by a greater efficacy of newer antidepressants, shown in studies of lower level of proof. Examining carefully the results of the 22 studies comparing the efficacy of older antidepressants to that of BZD, we observed no clear trend. Thus, an extrapolation by comparing the efficacy of newer to that of older antidepressants in head-to-head studies, as well as the respective efficacy of older and newer antidepressants to that of placebo does not seem to bring new information. In two open studies, the newer antidepressants sertraline and paroxetine had a slightly better efficacy than alprazolam and chlordesmethyldiazepam respectively.[9,10] Nevertheless, a singleblind methodology is not a high level of proof. Based on the above comments, the change from BZD to newer antidepressants was not based on efficacy data. Another possible explanation for the change from BZD to newer antidepressants, as far as efficacy is concerned, could have been the absence of clinical trials comparing efficacy of BZD to that of placebo in the recent years. However, this is not the case, as attested by 61 double-blind trials from 1990 to 2006.
Pharmacodependence
Pharmacodependence to BZD is a well known side-effect of BZD that was first described in medical literature in the sixties.[11] This was followed many years later by restrictions of treatment duration. Although SSRIs also cause discontinuation symptoms upon withdrawal, they are not considered as causing dependence and there are no craving symptoms. Fear of BZD dependence seems to be among the most often quoted reasons to shift from BZD to SSRIs. However, as with efficacy comparisons, there is a lack of safety comparisons conducted in a rational, evidencebased manner.
Although BZD are frequently prescribed in anxiety disorders, they cannot be considered as a first line treatment because of the risk of dependence. Despite this risk, BZD might be a second choice in anxiety disorders for patients who have suffered from SSRI inefficacy or side effects.
Benefit/Risk Ratio
The evaluation of the benefit/risk ratio, with high level of proof direct comparisons, should be the key-element in the decision-making process. In several guidelines where SSRIs are suggested over BZD on safety grounds, there is no mention to well-documented safety concerns of SSRIs, such as inappropriate ADH secretion syndrome, fatal hyponatremia, tardive dyskinesias, and other disabling extrapyramidal sideeffects, or SSRI-induced suicide attempts. Missing safety comparisons cannot be explained by missing safety data on SSRIs. For example, SSRI-induced suicide attempts were described as early as 1990,[12] and strong evidence suggesting a causal link was published two years later, with cases of positive dechallenges and even a positive rechallenge.[13]
Marketing
Marketing strategies must have played an important role in the occurrence of this change. Indeed the change opened a new market for antidepressants that cost more than BZD.
Registration Procedures
Since August 2006, an active comparator trial arm, as well as a withdrawal study, is requested by the European Medicines Agency in clinical investigation for the treatment of social anxiety disorder and generalized anxiety disorder. Such demands are not as clearly expressed for the treatment of panic disorder, and the guidelines are still being elaborated for the treatment of post-traumatic stress disorder.[14-16] Previous registration requirements obviously did not constrain the pharmaceutical industries to conduct clinical trials with direct comparisons between BZD and newer antidepressants in anxiety disorders.
Subjective Variables in the Decision-making Process
A tendency to prefer therapeutic novelty to long-proven therapies may have also contributed to the change. Indeed new drugs are sometimes prescribed more than justified by medical needs.[17-19] Emotional aspects play a role in risk analysis and in the decision-making process. Moreover, risk and benefit are negatively correlated in people’s judgments.[20] These cognitive bias or cognitive illusions might have to be taken into consideration.
Conclusion
The change from prescribing mainly BZD to prescribing mainly newer antidepressants in anxiety disorders was not based on solid evidence concerning comparative efficacy. This example of a worldwide change of prescribing pattern in absence of adequate comparative data has implications on the practice of medicine. Similar situations might exist in other fields of medicine.
Acknowledgements
Salaries of all authors came from the state of Geneva University Hospital. PS has acted as a paid consultant for the pharmaceutical industry and has accepted paid speaking engagements in industry supported symposia. PB, DH, IDD collected the data. PB, DH, RT, PS interpreted the data and drafted the manuscript. All authors participated in the critical revision of the manuscript and approved the final report.
No comments:
Post a Comment