- dr. Stanciu
- dr. Neacsu
- dr. Codreanu
Dubai
- Dr. Simu
- dr. Zamfirecu
- dr. Radescu
- dr. Solomon
- dr. Badea.
- dr. Bizamcer
- dr. Falculete
- dr. Dima
- dr. Stroe
- dr. Teodoru
- dr. Stuparu
- dr. Vlad M.
- dr. Cosma +
- dr. Stancu +
- dr. David
- dr. Tudor+
- dr. dela Fiziologie+
Dubai
September 11, 2008 (Rome, Italy) — Lifestyle changes, not drugs, should be the main focus for preventing type 2 diabetes: that was the conclusion of a lively debate here at the European Association for the Study of Diabetes 2008 Meeting. While Dr Paul Zimmet (Baker IDI Heart and Diabetes Institute, Melbourne, Australia) argued nimbly that glucose-lowering drugs could play an important role in preventing progression to diabetes, the audience, in a show of hands, ultimately voted to feed him to the lions following what both speakers, in a nod to their Roman surroundings, called a "gladiatorial debate."
In defense of lifestyle interventions, Dr Nick Wareham (Institute of Metabolic Science, Cambridge, UK), pointed to the fundamental, philosophical problem of treating patients who have no overt disease with pharmaceutical agents that have no proven benefits as preventive medications.
"As a physician I know that drug therapy is hugely beneficial in certain circumstances. The question is whether it is beneficial for people who don't have a disease to be treated with drugs," Wareham said. "I do not contest the notion that this group is at risk, but I think there is a profound philosophical question we're facing: when we as physicians seek out people who don't come to us to offer them help, we'd better be damn sure that what we're doing is actually going to do so."
But taking the counterposition, Zimmet cited the American Diabetes Association (ADA) consensus panel guidelines for people with impaired fasting glucose and impaired glucose tolerance, pointing out that while lifestyle changes are recommended, the writing group also "goes straight to metformin" in the presence of a wide range of risk factors common in the general population, relating to age, weight, family history, blood pressure, and lipid parameters. "This is a basic rejection of the idea that lifestyle alone works," Zimmet said.
Indeed, citing the ProACTIVE UK study, for which his opponent was an investigator, Zimmet pointed out that Wareham's own paper acknowledged that "it's very, very hard" to achieve a lifestyle intervention. In ProACTIVE UK, a behavioral intervention was no more effective than an "advice leaflet" for promoting physical activity in an at-risk group [1].
Forces Work Against Lifestyle
Backing up this claim, Zimmet showed a photograph of people attending the ADA annual meeting crammed onto escalators, while the stairs stood empty. "If we can't get the people pushing for lifestyle interventions to use the stairs themselves, then we really have a problem," Zimmet quipped.
Zimmet pointed to environmental, cultural, economic, and sociopolitical forces that work against lifestyle changes in developed countries, many of which are amplified in other parts of the world. "I'm a strong believer that lifestyle interventions can work, but maybe only in Alcatraz, where you can put people in prison and then rigorously control their exercise and diet regimen," he said.
If we can't get the people pushing for lifestyle interventions to use the stairs themselves, then we really have a problem.
The real reason, Zimmet reminded the audience, for preventing onset of type 2 diabetes is to reduce the risk of cardiovascular disease, but as he points out, "the clock starts ticking long before the line we actually call diabetes." And whether lifestyle changes alone will be enough to alter long-term effects remains unproven. In the 20-year follow-up from the Da Qing diabetes study, Zimmet noted, any significant differences between lifestyle intervention and control groups for cardiovascular or all-cause mortality that were apparent up to 14 years had disappeared after two decades [2].
But referring to the same study in his counterargument, Wareham pointed out that the Da Qing study was underpowered to detect these kinds of late-term differences, and, if anything, the totality of data overwhelmingly suggests that the effects of lifestyle interventions, once stopped, are far more durable than those of drugs. Zimmet had anticipated this point and suggested that the solution would be to just to stay on the drugs. Wareham, however, cited a comparison of lifestyle interventions and metformin by Herman et al, arguing that lifestyle changes are significantly more cost-effective in the first few years and, extrapolating over a lifetime, incur negligible costs per quality-associated life-year gained [3].
But perhaps most important, Wareham pointed out, lifestyle changes actually tackle the root cause of type 2 diabetes, not its consequences. And not only are they effective at reducing diabetes risk, Wareham noted, but they also have "halo effects," including anthropometric, physiological, metabolic, psychological, behavioral, and quality-of-life benefits.
Drugs, by contrast, may effectively reduce diabetes risk but often have adverse effects on some of these other factors and in some cases may actually have the effect of discouraging people from making meaningful lifestyle changes," Wareham argued.
Asked during the question period whether he had any specific recommendations for clinicians, Wareham acknowledged that a public-health problem requires sweeping changes in public-health policies--a point that both gladiators agreed upon. And conceding a point to Zimmet on the lack of long-term, hard-end-point studies for specific, clinically applicable lifestyle interventions, Wareham called for any funding agency representatives in the audience to sit up and take notice.
Controlling Risk Factors and Public Health Solutions
Before we embark on pharmacological therapy I would ask you whether you are doing that on the basis of evidence, or on assumption.
In his concluding remarks, Zimmet emphasized that in the future "preventive genomics" may prove useful for identifying individuals who could benefit from lifestyle changes and those in whom pharmacotherapy is appropriate. He also underscored the need for optimal control of other risk factors--lipids and blood pressure, through drugs as well as lifestyle--for preventing future disease.
For the time being, Zimmet concluded, "We must consider all options for prevention and drugs that are likely to magnify the benefit obtained from attempts at lifestyle measures."
Wareham, for his part, reiterated that the "true solution" to the problem of type 2 diabetes will be a public-health solution that encompasses transportation, school and workplace characteristics, and family activity levels and influences personal attitudes and choices. But in the meantime, he stressed, "before we embark on pharmacological therapy, I would ask you whether you are doing that on the basis of evidence or on assumption. There is evidence supporting lifestyle interventions. They can work, and they can be effective in the long term."
In a show of hands following the debate, Zimmet's prodrug arguments received a smattering of votes, while Wareham was the overwhelming winner.
Being Surer Than We Are
Speaking with heartwire after the debate, session cochair Dr Edwin Gale (Bristol University, UK) explained that while pharmacotherapy for type 2 diabetes prevention is "not really taking place" clinically, at present, it is a topic of major interest and debate among endocrinologists and diabetologists.
"We're looking closely at the evidence, because starting someone on a drug before they have a diagnosis is problematic. Impaired glucose intolerance is a soft diagnosis, because it can be made only with a glucose-tolerance test, and not many people are going to get this," he said. "I think that both speakers agreed that in the long term, it needs to be lifestyle changes for the whole population and not just directed at high-risk individuals. But we need better ways of identifying high-risk individuals, so we can intervene earlier."
Today, asymptomatic individuals typically undergo automatic glucose testing at age 45, Gale said, but he believes testing will start to be performed earlier, particularly in people with other diabetes risk factors, like obesity. "In reality, we will always start with lifestyle interventions, but if you see that someone is progressing toward diabetes, then you're going to start to see the use of drugs," he said.
But Gale reiterated that the evidence supporting a beneficial effect, in terms of hard diabetes and cardiovascular end points, of lowering glucose in people who are prediabetic, is lacking. And he agreed with Wareham that the creation of a label like "prediabetic," diagnosing a disease before it's present, is "a major worry." One issue, as both he and Zimmet suggested during the session, is that the definition of diabetes may need to be reconsidered so that people can be identified earlier in the disease process.
"This has to be risk-based treatment," Gale told heartwire, "and we have to have ways of being surer than we are at present that someone has risk before we start adding on drugs and changing their lives."
Objective: While there has been considerable concern over possible adverse effects of psychostimulants on brain development, this issue has not been examined in a prospective study. The authors sought to determine prospectively whether psychostimulant treatment for attention deficit hyperactivity disorder (ADHD) was associated with differences in the development of the cerebral cortex during adolescence. Method: Change in cortical thickness was estimated from two neuroanatomic MRI scans in 43 youths with ADHD. The mean age at the first scan was 12.5 years, and at the second scan, 16.4 years. Nineteen patients not treated with psychostimulants between the scans were compared with an age-matched group of 24 patients who were treated with psychostimulants. Further comparison was made against a template derived from 620 scans of 294 typically developing youths without ADHD. Results: Adolescents taking psychostimulants differed from those not taking psychostimulants in the rate of change of the cortical thickness in the right motor strip, the left middle/inferior frontal gyrus, and the right parieto-occipital region. The group difference was due to more rapid cortical thinning in the group not taking psychostimulants (mean cortical thinning of 0.16 mm/year [SD=0.17], compared with 0.03 mm/year [SD=0.11] in the group taking psychostimulants). Comparison against the typically developing cohort without ADHD showed that cortical thinning in the group not taking psychostimulants was in excess of age-appropriate rates. The treatment groups did not differ in clinical outcome, however. Conclusions: These findings show no evidence that psychostimulants were associated with slowing of overall growth of the cortical mantle.
Linmarie Sikich, M.D., Jean A. Frazier, M.D., Jon McClellan, M.D., Robert L. Findling, M.D., Benedetto Vitiello, M.D., Louise Ritz, M.B.A., Denisse Ambler, M.D., Madeline Puglia, B.A., Ann E. Maloney, M.D., Emily Michael, B.A., Sandra De Jong, M.D., Karen Slifka, R.N., C.S., Nancy Noyes, C.P.N.P., C.S., Stefanie Hlastala, Ph.D., Leslie Pierson, M.P.H., Nora K. McNamara, M.D., Denise Delporto-Bedoya, M.A., Robert Anderson, B.S., Robert M. Hamer, Ph.D., and Jeffrey A. Lieberman, M.D.
Objective: Atypical (second-generation) antipsychotics are considered standard treatment for children and adolescents with
early-onset schizophrenia and schizoaffective disorder. However, the superiority of second-generation antipsychotics over first-generation antipsychotics has not been demonstrated. This study
compared the efficacy and safety of two second-generation antipsychotics (olanzapine and risperidone) with a first-generation antipsychotic (molindone) in the treatment of early-onset schizophrenia
and schizoaffective disorder. Method: This double-blind multisite trial randomly assigned pediatric patients with early-onset
schizophrenia and schizoaffective disorder to treatment with either olanzapine (2.5–20 mg/day), risperidone (0.5–6 mg/day), or molindone (10–140 mg/day, plus 1 mg/day of
benztropine) for 8 weeks. The primary outcome was response to treatment, defined as a Clinical Global Impression (CGI) improvement score of 1 or 2 and  20% reduction in Positive and Negative Syndrome Scale (PANSS) total score after 8 weeks of treatment. Results: In total, 119
youth were randomly assigned to treatment. Of these subjects, 116 received at least one dose of treatment and thus were available for analysis. No significant differences were found among treatment
groups in response rates (molindone: 50%; olanzapine: 34%; risperidone: 46%) or magnitude of symptom reduction. Olanzapine and risperidone were associated with significantly greater weight gain.
Olanzapine showed the greatest risk of weight gain and significant increases in fasting cholesterol, low density lipoprotein, insulin, and liver transaminase levels. Molindone led to more
self-reports of akathisia. Conclusions: Risperidone and olanzapine did not demonstrate superior efficacy over molindone for treating
early-onset schizophrenia and schizoaffective disorder. Adverse effects were frequent but differed among medications. The results question the nearly exclusive use of second-generation
antipsychotics to treat early-onset schizophrenia and schizoaffective disorder. The safety findings related to weight gain and metabolic problems raise important public health concerns, given the
widespread use of second-generation antipsychotics in youth for nonpsychotic disorders
20% reduction in Positive and Negative Syndrome Scale (PANSS) total score after 8 weeks of treatment. Results: In total, 119
youth were randomly assigned to treatment. Of these subjects, 116 received at least one dose of treatment and thus were available for analysis. No significant differences were found among treatment
groups in response rates (molindone: 50%; olanzapine: 34%; risperidone: 46%) or magnitude of symptom reduction. Olanzapine and risperidone were associated with significantly greater weight gain.
Olanzapine showed the greatest risk of weight gain and significant increases in fasting cholesterol, low density lipoprotein, insulin, and liver transaminase levels. Molindone led to more
self-reports of akathisia. Conclusions: Risperidone and olanzapine did not demonstrate superior efficacy over molindone for treating
early-onset schizophrenia and schizoaffective disorder. Adverse effects were frequent but differed among medications. The results question the nearly exclusive use of second-generation
antipsychotics to treat early-onset schizophrenia and schizoaffective disorder. The safety findings related to weight gain and metabolic problems raise important public health concerns, given the
widespread use of second-generation antipsychotics in youth for nonpsychotic disorders
David J. Miklowitz, Ph.D.
Objective: Psychotherapy has long been recommended as adjunctive to pharmacotherapy for bipolar disorder, but it is unclear which interventions are effective for which patients, over what intervals, and for what domains of outcome. This article reviews randomized trials of adjunctive psychotherapy for bipolar disorder. Method: Eighteen trials of individual and group psychoeducation, systematic care, family therapy, interpersonal therapy, and cognitive-behavioral therapy are described. Relevant outcome variables include time to recovery, recurrence, duration of episodes, symptom severity, and psychosocial functioning. Results: The effects of the treatment modalities varied according to the clinical condition of patients at the time of random assignment and the polarity of symptoms at follow-up. Family therapy, interpersonal therapy, and systematic care appeared to be most effective in preventing recurrences when initiated after an acute episode, whereas cognitive-behavioral therapy and group psychoeducation appeared to be most effective when initiated during a period of recovery. Individual psychoeducational and systematic care programs were more effective for manic than depressive symptoms, whereas family therapy and cognitive-behavioral therapy were more effective for depressive than manic symptoms. Conclusions: Adjunctive psychotherapy enhances the symptomatic and functional outcomes of bipolar disorder over 2-year periods. The various modalities differ in content, structure, and associated mediating mechanisms. Treatments that emphasize medication adherence and early recognition of mood symptoms have stronger effects on mania, whereas treatments that emphasize cognitive and interpersonal coping strategies have stronger effects on depression. The placement of psychotherapy within chronic care algorithms and its role as a preventative agent in the early stages of the disorder deserve investigation.
News Author: Marlene Busko
CME Author: Charles Vega, MD
Disclosures
|
Physicians - maximum of 0.25 AMA PRA Category 1 Credit(s)™ for physicians
|
September 8, 2008 — A new international consensus statement on bipolar depression summarizes the most recent knowledge about this condition in children and adults, from epidemiology to treatment challenges and research design.
The statement, presented at the 21st European College of Neuropsychopharmacology (ECNP) Congress, in Barcelona, Spain, is based on discussions held in March 2007 including some 60 experts in bipolar disorder. The document was published in the July issue of European Neuropsychopharmacology and is available on the ENCP Web site.
"The profile of bipolar depression has assumed increasing importance," lead author, Guy M. Goodwin, BM, BCh, from the department of psychiatry at Warneford Hospital, in Oxford, the United Kingdom, told Medscape Psychiatry. "We hope to achieve awareness into how and why bipolar depression develops in young people and stimulate research into treatment."
The writing group includes participants from Australia, France, Germany, the Netherlands, Spain, the United Kingdom, and the United States and builds on an earlier document issued in 2001.
Diagnosis and Epidemiology
European surveys and a recent American survey estimate that, at some point in their lives, almost 2% of the population is affected by bipolar disorder and up to 6% by bipolar spectrum disorder.
Converging evidence suggests that the first onset of bipolar mood disorder occurs in the mid-teens to 20s until the 30s, when it usually manifests as a major depressive episode or hypomania. The onset of major depressive disorder tends to be later, and the risk continues into old age, which may reflect different causation for the 2 disorders.
"The early onset of bipolar disorder potentially implies a severe burden of disease in terms of impaired social and neuropsychological development, most of which is attributable to depression," the group emphasizes. Patients experience a debilitating decrease in functioning not only during their acute stages of illness, but increasingly also between episodes.
Bipolar disorder without depressive disorder is very rare, and the long-term course of bipolar disorder is dominated by depression rather than manic symptoms.
Since reliable criteria for delineating unipolar and bipolar depression are currently lacking, there is a considerable risk — probably over 10% — that patients initially diagnosed as having unipolar depression turn out have bipolar depression in the long run, the group stresses.
Bipolar Depression in Children
It is widely accepted that bipolar disorder exists in children and adolescents, but the age at which it can be first diagnosed remains controversial. Although bipolar-like symptoms may be quite frequent, reliably defined bipolar I disorder is rare in prepubertal children. Bipolar I disorder is characterized by a history of at least 1 manic episode, with or without depressive symptoms, whereas bipolar II disorder includes the presence of both depressive symptoms and a less severe form of mania, hypomania.
Early-onset bipolar disorder is increasingly recognized when patients are in their late teens. Since early intervention may improve patients' prognosis, trials of treatments for children and adolescents are important, the consensus document notes. To determine the best treatments, rather than extrapolate findings from clinical trials in adult patients, clinical trials are needed for young patients. It remains a challenge to find ways to collaborate and recruit patients for such research studies.
"The ECNP supports collaborating networks of clinicians in Europe who seek to improve treatment and research in children" with bipolar disorder," the group writes.
Bipolar Depression vs Unipolar Depression in Adults
Currently, the Diagnostic and Statistical Manual of Mental Disorders, 4th ed (DSM-IV) criteria for a major depressive episode in bipolar depression (or unipolar depression) do not take into consideration the overall course of the disorder. The next edition of the DSM is likely to use a probabilistic definition, as recommended by the International Society for Bipolar Disorders, to distinguish bipolar from unipolar depression, and this type of definition should be used in future research studies, they write.
Since anxiety is commonly present in bipolar populations, randomized controlled trials should accept patients with comorbid anxiety. Rapid cycling patients, defined as having 4 or more episodes a year, can also be recruited into these trials without impairing the outcomes.
Treatment Studies
Monotherapy trials comparing a drug vs placebo remain the gold-standard clinical-trial design for determining efficacy in bipolar depression. If efficacy is proven for a new drug vs placebo, the drug can then be tested in a placebo-controlled trial with adjunctive medication, the authors write. Younger adults, without an established need for long-term medication, may be particularly suited to placebo-controlled clinical trials.
The minimum scores for entry into bipolar-depression trials should be more than 20 on the Hamilton-Depression (HAM-D) 17-item rating scale, and efficacy is best detected in patients with a HAM-D rating more than 24 at baseline, they recommend.
In addition to basing trial outcomes on ratings in the traditional symptom-severity scales, it would be advisable to include secondary measures of functionality, such as quality-of-life measures and neuropsychological tests of attention, memory, and executive function.
Preventing Switch to Mania
"Switching from bipolar depression to mania or hypomania is a particular risk that requires a different approach to treatment from unipolar depression," the group cautions.
Some medications, such as the tricyclic antidepressants and venlafaxine, may be more likely than other medications to provoke this switch, but this effect might not be seen until 10 weeks of treatment. Thus, 12-week trials of drug vs placebo are needed to determine the risk for switch and to establish continuing effects, they write.
Study subjects need to be assessed carefully at 6 to 8 weeks to ensure nonresponsive patients do not remain in the study for an unacceptable length of time.
Preventing Relapse
"Long-term prevention of relapse is the major challenge in bipolar disorder. Success requires a mature therapeutic alliance between doctor and patient, effective self-management by the patients and their families, and effective, well-tolerated treatments," the group notes.
Trials that aim to detect a maintenance effect or a continued response should follow a relapse-prevention design. That is, patients who are experiencing an episode of bipolar disorder are treated with a study drug and are then randomized to continue active treatment with the drug or to receive placebo. However, acute withdrawal of active medication after treatment response might artificially enhance the effect of the study drug, they note.
A short tapering-off period is usually desirable. In addition, mood stabilization for up to 3-month periods is desirable, but protocol compliance for these longer periods may be difficult to achieve, making these studies more expensive and more difficult to conduct.
Clinical trials that include the addition of a drug to other agents during or after the resolution of a depressive or manic episode and then investigate the effect of this drug vs placebo to prevent relapse would be clinically informative.
Clinical Challenge
In the United States, as compared with Europe, "there are no differences in the clinical challenge — it's the same disease — but healthcare systems are different, and this affects patient access," said Dr. Goodwin. "The United States has gone much further in trying to diagnose children before an adult pattern of illness is present. This is a hazardous project, and the European approach is more cautious."
We performed a systematic review of controlled trials on anxiety disorders treatment (generalized anxiety disorder, panic disorder, social phobia and post-traumatic stress disorder) published from 1980 to 2006, and identified trials comparing the efficacy of benzodiazepines (BZD) with that of antidepressants, in particular comparisons between BZD and newer antidepressants. Among 969 publications, 274 double-blind randomized controlled studies remained after using our exclusion criteria. These studies comprised altogether 439 comparisons. There were in total 23 comparisons of antidepressants versus BZD. Among these, 22 compared the efficacy of older antidepressants versus BZD, whereas only 1 concerned the comparison of a newer antidepressant versus BZD. It showed comparable efficacy between venlafaxine and diazepam in the treatment of generalized anxiety disorder. Our study shows that the major change of prescribing pattern from BZD to newer antidepressants in anxiety disorders has occurred in absence of comparative data of high level of proof.
In the last decade, there was an important shift of prescribing pattern from BZD to newer antidepressants, with an almost 3-fold increase of the prescriptions of the latter. This increase exceeds that for depression diagnosis.[1,2]
There was also a shift in the expert opinions; in two surveys among experts in anxiety disorders, a clear change of preferences was noted, from BZD in 1992 to newer antidepressants in 1997.[3] In evidence-based medicine, when two or more options of treatment are available, the decision-making process should ideally be based on direct comparison of efficacy and side-effects.We examined a sample of expert opinions and psychiatric guidelines. In the treatment of anxiety disorders, both BZD and antidepressants were recognized as efficacious and the risk of dependence to BZD was evoked. However, neither experts nor guideline panels mentioned trials with direct comparisons (of efficacy or side-effects) between BZD and newer antidepressants.[3,5,6]
Hence, we formulated the hypothesis that the major change of prescribing pattern may have occurred in absence of adequate comparative evidence of efficacy, i.e., randomized controlled trials with direct comparison between newer antidepressants and BZD in anxiety disorders. The objective of this study was to assess if this comparative evidence indeed exists
We performed a systematic review of the literature on the pharmacotherapy of anxiety disorders, using a reproducible Medline search syntax (available from the authors). Studies on the pharmacotherapy of anxiety disorders, comprising at least one arm with benzodiazepines or antidepressants, were included. Tricyclic/tetracyclic antidepressants and monoamine oxidase inhibitors were grouped under the label of older antidepressants. SSRIs and other recent antidepressants were grouped under the label of newer antidepressants (Table 1).
We set limits to publication dates from 1980 to 2006, to randomized controlled trials, and human trials. Studies with the following characteristics were excluded manually after the Medline search: methodology other than double-blind randomized controlled trial; non-pharmacological comparators (e.g., cognitive behavioral therapy) as well as trials with neither BZD, nor antidepressants in monotherapy as an arm (e.g., discontinuation and augmentation studies); redundant data (e.g., duplicate publications, analyze of subgroups); provoked panic attacks in experimental conditions (e.g., lactate, carbon dioxide); language of publication other than English; and diagnosis other than panic disorder, generalized anxiety disorder, social phobia and post-traumatic stress disorder (e.g., obsessive-compulsive disorder, depression with anxious symptoms, other specific phobia, anxious syndrome unspecified). Obsessive-compulsive disorder is not recognized as an indication for primary treatment using a BZD and was therefore not included in our study. Studies with several clinical entities were classified according to the diagnosis of the greater number of patients. The vast majority of excluded studies did not meet diagnosis criteria; many of them met two or more exclusion criteria.
We listed the trials comparing the efficacy of BZD with antidepressants, in particular those concerning newer antidepressants. We also listed the comparisons between antidepressants and placebo, BZD and placebo, antidepressants and antidepressants, BZD and BZD, and antidepressants/BZD and another compound.
We listed comparisons rather than only trials, since a given trial may comprise several comparisons.
We identified 969 publications, when the search syntax was performed in January, 2007. After exclusions, 274 double-blind randomized controlled studies remained (the complete list of references for the trials selected can be obtained from the first author). These studies comprised altogether 439 comparisons. Panic disorder was the entity with the highest number of trials, i.e., 110 double-blind randomized comparative trials containing 170 comparisons, during a 27-year period. Generalized anxiety disorder was next, with 87 trials containing 174 comparisons.
There were in total 23 comparisons of antidepressants versus BZD. Among these, 22 compared the efficacy of older antidepressants versus BZD (Figure 1), whereas only 1 concerned the comparison of a newer antidepressant versus BZD.[7] It showed comparable efficacy between venlafaxine and diazepam.
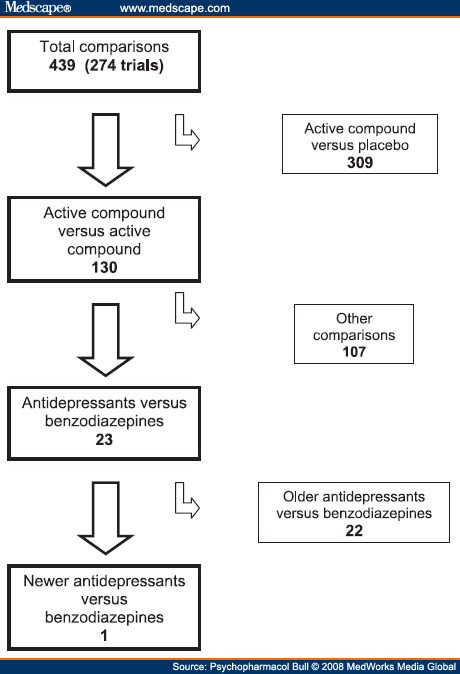 |
Figure 1. (click image to zoom) Number of double-blind comparisons in randomized controlled trials on pharmacological treatment of anxiety disorders.
|
We also found 183 comparisons between antidepressants and placebo (113 concerning newer antidepressants) and 90 comparisons between BZD and placebo. Also, 86 comparisons concerned an antidepressant or a BZD versus other compounds, or other compounds versus placebo. There were a total of 309 comparisons where the comparative compound was placebo, i.e., more than 70%. Antidepressants were compared to antidepressants 37 times and BZD were compared to BZD 20 times. Table 2 gives the overview as to the number of comparisons for each anxiety disorder and for each category of comparisons
Our study clearly shows that the change of prescribing pattern from BZD to newer antidepressants was not based on evidence of a high level of proof, since there is only one double-blind, randomized controlled trial comparing one of these antidepressants to a BZD, among 274 double-blind, randomized controlled trials on drug efficacy in panic disorder, generalized anxiety, social phobia and post-traumatic stress disorder. This single study is that of Hacket and collaborators, about the efficacy of venlafaxine XR and diazepam in generalized anxiety disorder.[7] No statistically significative difference was found between these two compounds. In other words, a major change of prescribing pattern from BZD to newer antidepressants has occurred all around the world in the absence of comparative studies with a high level of proof. Such a situation is surprising, considering that the declaration of Helsinki insists on the fact that, if a comparative compound is available, it should be used in clinical trials of new molecules. It is stated in the article 29 of the Declaration of Helsinki that "the benefits, risks, burdens and effectiveness of a new method should be tested against those of the best current prophylactic, diagnostic and therapeutic methods."[8] Various reasons, not mutually exclusive, could explain this change of prescribing pattern.
The change from BZD to newer antidepressants may have been in the interest of the patients, but this remains to be proven with studies of high level of proof. Nevertheless, the change from BZD to newer antidepressants could be explained by a greater efficacy of newer antidepressants, shown in studies of lower level of proof. Examining carefully the results of the 22 studies comparing the efficacy of older antidepressants to that of BZD, we observed no clear trend. Thus, an extrapolation by comparing the efficacy of newer to that of older antidepressants in head-to-head studies, as well as the respective efficacy of older and newer antidepressants to that of placebo does not seem to bring new information. In two open studies, the newer antidepressants sertraline and paroxetine had a slightly better efficacy than alprazolam and chlordesmethyldiazepam respectively.[9,10] Nevertheless, a singleblind methodology is not a high level of proof. Based on the above comments, the change from BZD to newer antidepressants was not based on efficacy data. Another possible explanation for the change from BZD to newer antidepressants, as far as efficacy is concerned, could have been the absence of clinical trials comparing efficacy of BZD to that of placebo in the recent years. However, this is not the case, as attested by 61 double-blind trials from 1990 to 2006.
Pharmacodependence to BZD is a well known side-effect of BZD that was first described in medical literature in the sixties.[11] This was followed many years later by restrictions of treatment duration. Although SSRIs also cause discontinuation symptoms upon withdrawal, they are not considered as causing dependence and there are no craving symptoms. Fear of BZD dependence seems to be among the most often quoted reasons to shift from BZD to SSRIs. However, as with efficacy comparisons, there is a lack of safety comparisons conducted in a rational, evidencebased manner.
Although BZD are frequently prescribed in anxiety disorders, they cannot be considered as a first line treatment because of the risk of dependence. Despite this risk, BZD might be a second choice in anxiety disorders for patients who have suffered from SSRI inefficacy or side effects.
The evaluation of the benefit/risk ratio, with high level of proof direct comparisons, should be the key-element in the decision-making process. In several guidelines where SSRIs are suggested over BZD on safety grounds, there is no mention to well-documented safety concerns of SSRIs, such as inappropriate ADH secretion syndrome, fatal hyponatremia, tardive dyskinesias, and other disabling extrapyramidal sideeffects, or SSRI-induced suicide attempts. Missing safety comparisons cannot be explained by missing safety data on SSRIs. For example, SSRI-induced suicide attempts were described as early as 1990,[12] and strong evidence suggesting a causal link was published two years later, with cases of positive dechallenges and even a positive rechallenge.[13]
Marketing strategies must have played an important role in the occurrence of this change. Indeed the change opened a new market for antidepressants that cost more than BZD.
Since August 2006, an active comparator trial arm, as well as a withdrawal study, is requested by the European Medicines Agency in clinical investigation for the treatment of social anxiety disorder and generalized anxiety disorder. Such demands are not as clearly expressed for the treatment of panic disorder, and the guidelines are still being elaborated for the treatment of post-traumatic stress disorder.[14-16] Previous registration requirements obviously did not constrain the pharmaceutical industries to conduct clinical trials with direct comparisons between BZD and newer antidepressants in anxiety disorders.
A tendency to prefer therapeutic novelty to long-proven therapies may have also contributed to the change. Indeed new drugs are sometimes prescribed more than justified by medical needs.[17-19] Emotional aspects play a role in risk analysis and in the decision-making process. Moreover, risk and benefit are negatively correlated in people’s judgments.[20] These cognitive bias or cognitive illusions might have to be taken into consideration.
The change from prescribing mainly BZD to prescribing mainly newer antidepressants in anxiety disorders was not based on solid evidence concerning comparative efficacy. This example of a worldwide change of prescribing pattern in absence of adequate comparative data has implications on the practice of medicine. Similar situations might exist in other fields of medicine.
Salaries of all authors came from the state of Geneva University Hospital. PS has acted as a paid consultant for the pharmaceutical industry and has accepted paid speaking engagements in industry supported symposia. PB, DH, IDD collected the data. PB, DH, RT, PS interpreted the data and drafted the manuscript. All authors participated in the critical revision of the manuscript and approved the final report.
Cognitive function and mental illness
The various elements of cognitive function lie at the core of psychiatric illness. Several papers in this issue of the Journal examine the contribution of cognition to a range of signs and symptoms of illness. There is an increasing awareness of the presence of a continuum of psychotic symptoms within the general population, and that symptoms in childhood, within this non-clinical population, may be predictive of a schizophreniform illness in later life. Horwood and colleagues (pp. 185–191) found that psychotic symptoms were reported by a significant proportion of 12-year-old children, 13.7% reporting at least one symptom over a 6-month period, and the prevalence was highest in those with lower IQ scores, contributed to mainly by the verbal IQ. The authors concluded that self-report questionnaires were inadequate for screening for symptoms, as they tended to inflate the prevalence figures, and that although psychotic symptoms are relatively common in childhood, the relationship with IQ differs from that seen later in schizophrenia, and thus different mechanisms appear to be at play. Dazzan et al (pp. 197–202) examined neurological soft signs and cognitive ability in a sample of people with first-episode schizophrenia and showed increased rates of a range of soft signs in schizophrenia compared with control participants; however, when matched for IQ, only primary signs and motor coordination appeared specific to the presence of psychosis. Fullam & Dolan (pp. 247–253) demonstrate that neuropsychological variables such as executive function did not distinguish between in-patients with schizophrenia who had been violent and those who had not. They suggest that personality factors such as psychopathy and low current IQ may be more important in understanding in-patient violence.
Cognitive–behavioural therapy: depression and PTSD
The cost of delivering CBT is often seen as skewing the cost–benefit ratio, and therefore there has been interest in using technology, particularly computerised CBT, to reduce these costs. Kaltenthaler et al (pp. 181–184) performed a systematic review of computerised CBT for depression and conclude that three out of four trials showed evidence of effectiveness. However, they expressed some concerns about the self-selected nature of the participants and lack of adequate data on drop-out rates and raise the issue of effectiveness in a more representative group of patients. Wild & Gur (pp. 254–255) examined whether memory deficits in post-traumatic stress disorder could influence treatment outcome. They report that patients with poor verbal memory were less likely to respond to a course of CBT. The authors suggest that these patients may require additional cues to aid their progress, or could perhaps be considered for other treatment modalities, such as eye movement desensitisation reprocessing, which has a lower verbal memory demand.
Psychosis: white matter, duration of untreated illness and social functioning
Schizophrenia is considered to be a disorder of brain connectivity and Walterfang and colleagues (pp. 210–215) examined white matter in the brains of individuals considered to be at high risk of developing a psychotic illness. They found that people who later developed psychosis had increased white matter in their frontal cortex at baseline imaging, and demonstrated a progressive reduction in the white matter of the fronto-occipital fasciculus. They suggest that this may be indicative of changes in the connectivity between the frontal and temporal, parietal and occipital regions that are connected by these tracts. Barnes et al (pp. 203–209) addressed the role of duration of untreated psychosis (DUP) in social functioning of patients 1 year after presenting with a first episode of schizophrenia. They hypothesised that the relationship between these would be mediated by the level of symptomology. Although they did find the expected relationship between a longer DUP and poorer social function, this was independent of the level of symptoms, as a longer DUP was also predictive of poorer clinical outcome with more persistent symptoms at follow up.
Ethnicity: carers and prescribing antidepressants
The majority of people with dementia are looked after in the community, often with considerable support from family members. This is especially so in Black and minority ethnic populations, who tend to be less likely to access services. Lawrence and colleagues (pp. 240–246) pose the question – what is the best way of supporting these carers? They identified that carers’ attitudes could be used to divide them into two groups: first, those with traditional beliefs, exemplified by implicitly prioritising the patient’s needs over their own, and viewing the seeking of professional help as a failure to fulfil their own responsibilities; and a second group with non-traditional beliefs. The majority of south Asian carers, half the Black Caribbean and the minority of White British participants held the traditional ideology. The authors suggest how different approaches will be necessary to support these different carer profiles.
The WPA position statement on the ethics of the use of unmodified electroconvulsive therapy
Prepared by the WPA Standing Committee on Ethics and the WPA Section of Biological Psychiatry
This position statement is an addendum to the one on the use and safety of electroconvulsive therapy that was prepared by the Section of Biological Psychiatry in 2004 and was eventually approved by the WPA General Assembly in 2005 (WPA Position Statement, 2004).
Introduction
The WPA position statement on the use and safety of ECT has referred to ethical considerations in its use; the need to obtain informed consent from those with capacity to consent; to ensure that the patients’ relatives and carers are consulted in the case of patients with impaired capacity to consent and to seek a second opinion from an appropriately trained professional. However, the statement has not dealt specifically with the use and safety of unmodified ECT or the ethics of its practice. It is to be noted in this context that most national guidelines on the use of ECT have not referred to the use of unmodified ECT. This may be related to the notion that unmodified ECT is hardly ever used in Western Europe, North America and Australasia, countries that have produced these national guidelines. The WPA, as a global health professional organisation, needs to provide guidance on the use of unmodified ECT, in view of the continued use of this method in many countries.
Electroconvulsive therapy, which was introduced in 1938, was originally unmodified and involved the administration of electrical current resulting in a generalised convulsion. Injuries resulting from violent convulsions were prevented by applying physical restraint and holding of the patient. ECT induces a central seizure detected by eletroencephalogram and a visible convulsion. All along, it was conceived that the central seizure and the peripheral convulsion were the effective ingredients in ECT. The ECT procedure was modified in the 1950s with the introduction of anaesthesia and muscle relaxation prior to the administration of ECT. In addition, patients were premedicated with atropine, administered subcutaneously 30-60 minutes before the ECT, to reduce bronchial secretions and inhibit the vagal discharge which accompanies the convulsion and thus minimise the occurrence of arrhythmias. In view of the cerebral effects of atropine it was later replaced by methylscopolamine, which does not cross the blood-brain barrier.
For anaesthesia, short acting barbiturates such as methylhexitone or thyopentone are used at the minimal dose so that the seizure threshold is not raised. The dose should be sufficient to induce unconsciousness to prevent the terrifying experience of total paralysis, including paralysis of respiratory muscles, induced by the muscle relaxant.
Once the patient is rendered unconscious, the muscle relaxant (suxamethonium), the modifying agent with the effect of abolishing the peripheral convulsion, is introduced. Once the anaesthetic and the muscle relaxant are given, 100% oxygen is administered by mask before and after the convulsion and continued until spontaneous respiration has returned. The safe administration of ECT requires the involvement of an anaesthetist or other appropriately trained health practitioners such as psychiatrists or nurses.
The use of unmodified ECT has been variously described as barbaric, inhumane and unethical, labels that have also been used to describe ECT whether modified or unmodified. In the case of unmodified ECT, this derives from the impression of the onlookers witnessing the patient whilst having a generalised convulsion and being physically held and restrained to prevent physical injury. With the introduction of modified ECT, in the 1950s, the use of unmodified ECT was gradually phased out over the next two decades. Modified ECT has become the standard practice in Western Europe, North America and Australasia. However, reports and surveys have shown that unmodified ECT is still used in Japan, Russia,
* Our Turkish colleagues have reassured us that administration of unmodified ECT has ceased now.
China, India, Thailand , Turkey* and in many low and middle – income countries.
Concerns were expressed by the European Committee for the Prevention of Torture and Inhuman or Degrading Treatment or Punishment on the use of unmodified ECT in Turkey (http://www.cpt.coe.int/en/states/tur.htm). The Turkish Government has responded to the report indicating that it has taken corrective action (http://www.cpt.coe.int/documents/tur/2006-30-inf-eng.htm).
A recent survey of ECT practice in Japan reported the use of unmodified ECT in 60 institutions (Chanpattana, et al, 2005) and in 37 of these 60 institutions unmodified ECT was used exclusively, less in University than in non – University psychiatric hospitals. The reasons for using unmodified ECT included emergency, lack of anaesthetist and equipment, being “safer than modified ECT” and being reserved for young people. Particular side - effects of unmodified ECT included incidence of teeth injury, arrthymia and fracture/dislocation. No cases of ECT – related death were reported.
A national survey of ECT use in the Russian Federation reported that fewer than 20% of ECTs were modified with anaesthesia. Anaesthesia and muscle relaxants were never used in 31 out of the 42 responding institutions, estimating that 21% of institutions used modified ECT at least sometimes (Nelson, 2005). It was noted in the report that there was no system or expectation for ECT training and no national organisation to advance ECT practice despite the respondents’ enthusiasm and positive attitudes towards ECT and for adopting modern ECT methods.
The national Survey of ECT Practice in Thailand (Chanpattana and Kramer, 2004) showed that unmodified ECT was used always in 9 psychiatric and 5 general hospitals and occasionally in two university hospitals, comprising 94% of all ECT use. Respondents gave reasons for their use of unmodified ECT: lack of funds, convenience, lack of personnel, lack of equipment, lack of anaesthesia and economic reasons. This was related to the poor infrastructure and resourcing of mental health services and specifically to the psychiatrists’ attitudes and lack of training in the practice of ECT.
A survey of the practice of ECT in 188 teaching institutions and psychiatric hospitals in India, showed that more than 70% of ECT administrations were performed in psychiatric hospitals and approximately half of ECT use was on unmodified ECT (Chanpattana et al, 2005).
However, there are very few reports on the use of unmodified ECT from low income countries, except for earlier studies from Nigeria indicating that unmodified ECT was the main method of administration (Obejide et al, 1987; Ikeji et al, 1999). This is likely to be the case in many low income countries, in view of the poor infrastructure and funding for psychiatric services and the lack of trained mental health professionals.
There have been few controlled studies on the comparative efficacy of modified and unmodified ECT. Kendell (1981) reviewed the few controlled studies and concluded that modified and unmodified ECT were equally effective, as shown in the studies by Havens (1958) and Seager (1959) which both involved substantial numbers of patients who were randomly allocated to the two treatments. Further studies specifically evaluating the therapeutic effects of the convulsion confirmed it as the therapeutic ingredient (Ulett et al, 1956; Laurell, 1970; Ottosson, 1960). The role of the convulsion in mediating the therapeutic effects of ECT has, of course, been strongly supported by the controlled studies of real and simulated ECT reviewed in the WPA consensus statement on its use (2004).
The controversy over the use of unmodified ECT, however, has been mainly related to its risks and adverse effects. Not withstanding the recognised and well documented adverse effects of ECT, as reviewed in the WPA consensus statement, unmodified ECT has been associated with physical injuries produced by the uncontrolled convulsive movements which cause fractures in the mid thoracic vertebrae and dislocations particularly of the jaw, occurring in 30% of patients in some studies (Kendell, 1981). Andrade et al (2003) highlighted the disadvantages of unmodified ECT with reference to Western research conducted in the 1940s and 1950s which suggested that convulsions were associated with 20-40% risk of multiple subclinical vertebral body compression fractures, mostly affecting the middle thoracic vertebrae, observed mainly in males, in young and in old subjects. However, these fractures were not associated with pain or other symptoms and did not require orthopaedic intervention.
Andrade et al (2003) have reported new research on the adverse effects of unmodified ECT conducted in India between 1980 and 1990, reporting that only 0.7 % of patients had fractures with unmodified ECT, the majority of whom suffered no pain or disability or other musculoskeletal complications (Tharyan et al, 1993). A further study with radiological evidence showed 2% rate of vertebral injury (Andrade, et al, 2000). Unmodified ECT does not appear to cause internal tissue damage (Ohaeri et al, 1992).
It must be noted that unmodified ECT is essentially unmonitored ECT as well, meaning that all acquired knowledge as to the monitoring of the seizure and the related physiological parameters can not be used.
The principal ethical concern about the use of unmodified ECT is related to the risk of suffering the aforementioned adverse effects that do not occur when modified ECT is used. However, such risks should be set against the benefits of administration of unmodified ECT in cases where ECT is strongly indicated and can not be given in its modified form. Such a case is psychotic depression with high suicidal risk which requires rapid intervention with ECT, the most effective treatment in such a condition.
The pros and cons of administering unmodified ECT should be carefully considered. In any case, however, informed consent, including consent of the patient’s relatives and carers, should be secured. There needs to be an appreciation of the realities of practice of ECT in low income countries with poor service infrastructure and limited availability of anaesthetists and medication for the administration of modified ECT. It must be noted that there is no guidance on the use of unmodified ECT by the American Psychiatric Association, the Royal College of Psychiatrists and other authoritative bodies catering for ECT practice in high income and well resourced countries. The WPA as a global association of national psychiatric organisations strongly advocates the use of modified ECT as standard and optimal practice. However, it is recognised that there are cases in which psychiatrists are faced with the situation where ECT is strongly indicated but there are no facilities and skilled staff to administer it in its modified form. In these cases, unmodified ECT should be considered as an option after full consultation with the patients and their relatives and ensuring informed consent is obtained. Such considerations are no different from considerations of urgent medical and surgical interventions that may be associated with greater risks and more serious adverse effects.
Andrade et al (2003) in their commentary on the dilemma of unmodified ECT, referred to the civil rights activities in India which culminated in a non - governmental organisation for the rights of the mentally ill filing a petition to the supreme court of India in 2001 seeking a blanket prohibition of the practice of unmodified ECT. In relation to this, it is noted that the national psychiatric associations in India have advocated that, whilst the practice of modified ECT should be the rule, consideration should be given to exceptions when unmodified ECT should be considered. The verdict of the Supreme Court is still awaited. Andrade et al (2003) regretted that the Indian Psychiatric Society had not taken an official position on the use of unmodified ECT or produced guidelines to that effect and have advocated that “there are extenuating circumstances in which unmodified ECT may be better than no ECT …. and that the decision to administer unmodified ECT must be made in exceptional circumstances and on a case by case basis, and never as a routine practice …… “
Whilst unmodified ECT is as effective as modified ECT (administered with an anaesthetic and a muscle relaxant) it is associated with significant risk and adverse effects (fractures and dislocation) and with pre-treatment suffering of the patient which do not occur with modified ECT. This has rendered the use of unmodified ECT more controversial than modified ECT and raised ethical concerns over its continued use. Recent reviews of the practice of ECT have indicated that unmodified ECT is still in use in countries, mainly developing and of low income, with poor infrastructure and funding for mental health services and limited professional human resources. Understandably, guidances from National Professional Associations in Western Europe and the US have not tackled the issue of the use of unmodified ECT as it is no longer in use in these countries.
Regrettably the national psychiatric associations in countries where unmodified ECT is still in use, have not provided guidance on its use. The WPA, as a global professional association and following the International congress in Istanbul (2006) and the ECT Instanbul consensus Recommendations (2006) has issued this addendum statement on the use, safety and ethics of unmodified ECT and makes the following recommendations:
The National Member Societies of the WPA, in collaboration with their governments are asked to implement the WPA declarations, statements and guidelines on ethics and consider the recommendations of the WHO resource book on mental health, human rights and legislation, with the following aims:-
· To cease the use of unmodified ECT, in view of evidence indicating that this method has no difference in effectiveness from modified ECT but has more adverse effects.
References
Andrade, C., Rele, K., Sutharshan, R., Shah, N. (2000) Musculoskeletal morbidity with unmodified ECT may be less than earlier believed. Indian Journal of Psychiatry, 42: 156-162.
Andrade C. (2003) Unmodified ECT: ethical issues. Issues Med Ethics, 11(1): 9-10.
Andrade C, Shah N, & Tharvan, P. (2003) The dilemma of unmodified electroconvulsive therapy. Journal of Clinical Psychiatry, 64 (10); 1147-1152.
APA BOT Statement on the use of unmodified ECT, adopted in March 2007.
Chanpattana W, and Kramer BA, (2004) Electroconvulsive therapy practice in Thailand. J ECT, 20 (2): 94-98.
Chanpattana W, Kojima K, Kramer BA, Intakorn A, Sasaki S, Kitphati R. (2005) ECT practice in Japan. J ECT, 21 (3): 139-144.
Chanpattana W, Kunigiri G, Kramer BA, Gangadhar BN. (2005)
Survey of the practice of electroconvulsive therapy in teaching hospitals in India. J ECT. 2005 Jun;21(2):100-4.
ECT Instanbul Consensus Recommendations (prepared by C. Yazgan, R. Okin, Th. Bolwig, O. Steenfeldt-Foss, D. Yesibursa, J. McIntyre, S. Rataemane and E. Sorel) 2006.
Havens L. L. (1958) A comparative study of modified and unmodified electric shock treatment. Diseases of the Nervous System, 19: 1-6.
Ikeji OC, Ohaeri JU, Osahon RO, Agidee RO. (1999). Naturalistic comparative study of outcome and cognitive effects of unmodified electro-convulsive therapy in schizophrenia, mania and severe depression in Nigeria. East Africa Med J.;76(11):644-50.
Kendell, R. E. (1981) The present status of electroconvulsive therapy. British Journal of Psychiatry, 139: 265-283.
Laurell, B. (1970) Flurothyl convulsive therapy. Acta Psychiatrica Scandinavica, Suppl. 213.
Nelson, A. I. (2005) A national survey of electroconvulsive therapy use in the Russian Federation. J ECT, 21 (3): 151-157.
Odejide AO, Ohaeri JU, Ikuesan BA. (1987). Electroconvulsive Therapy in Nigeria. Convuls Ther. 1987;3(1):31-39
Ohaeri, J. U., Hedo, C. C., Envidah, S. N., Ogunnivi, A. O. (1992) Tissue injury inducing potential of unmodified ECT: serial measurement of acute phase reactants. Convuls. Therapy, 8 (4): 253-257.
Ottosson, J.O. (1960) Experimental studies of the mode of action of electroconvulsive therapy. Acta Psychiatrica Scandinavica, Suppl. 145.
Seager, C. P. (1959) Controlled trial of straight and modified electroplexy. Journal of Mental Science, 105: 1022-1028.
Tharyan, P., Saju, PJ., Datta, S., John, JK., Kuruvilla, K. (1993) Physical morbidity with unmodified ECT: a decade of experience. Indian Journal of Psychiatry, 35: 211-214.
Ulett, G. A., Smith, K. and Gleser, G. C. (1956) Evaluation of convulsive and subconvulsive shock therapies utilizing a control group. American Journal of Psychiatry, 112: 795-802.
WPA position statement on the use and safety of ECT (2004) Science and Care, Bulletin of the WPA Scientific Sections,1:7-11.
This statement was prepared my Mohammed Abou Saleh, it has been revised and edited by George Christodoulou, has been reviewed by the members of the WPA Standing Committee on Ethics and the WPA Section of Biological Psychiatry and has incorporated the comments of the WPA Member Societies and other WPA components. Special mention must be made of the contribution of Eliot Sorel and the WPA Section on Conflict Management and Resolution.
Submitted in August 2008
On behalf of the WPA Standing Committee on Ethics
Prof George Christodoulou
On behalf of the WPA Section on Biological Psychiatry
Prof Mohammed Abou-Saleh
This statement was prepared by the Standing Committee on Ethics of the W.P.A., in response to a request from the WPA Executive Committee.
Increased awareness of the pharmaceutical industry’s (henceforth referred to as “industry”) influence on the profession has led to a range of concerns and the need for guidance, supplementing the WPA Guidelines concerning support from external sources for activities of the WPA (1).
I. Purpose: 1) To clarify ways in which industry and
the profession interact.
2) To identify actions which may : undermine the agreed
upon values of the profession,
exert a negative effect on its autonomy
and interfere with a commitment to care optimally
for patients, based on well-grounded
research evidence.
3) To provide guidance to assist Psychiatrists
to maintain constructive links with industry at the
same time maintaining their autonomy.
II. Historical context
The growing association between industry and psychiatry has its roots not only in a deeper understanding of the nature of biological factors relevant to mental illness but also in the parallel expansion of pharmacological options available to the practitioner to limit suffering and disability.
Accompanying these developments has been the regular publication of peer-reviewed articles drawing attention to the multi-layered and complex relationship between industry and psychiatry and the ethical issues inherent in this relationship.
Industry is certainly committed to developing safe, effective drugs with fewer side-effects but it also has to satisfy its shareholders who
(1) Guidelines concerning support from external sources for activities of the World Psychiatric Association. Approved by the WPA General Assembly in Hamburgh on August 8, 1999. WPA Information Guide 2005 - 2008
naturally wish to see a maximum return on their investment. Therein lies a potential problem, as prescribers come under continuing pressure from a range of sources (including, more recently, informed patients and their families) to choose specific medications
IV. Brief review of what has been learned about the links between industry and psychiatry.
· Industry’s influence begins during psychiatric training through such features as token gifts, free meals and colleagues lecturing on behalf of a company, as well as through role-models. Many academic centers have instituted guidelines to address these influences but their number and distribution are relatively unknown.
· Clinicians, including psychiatrists, are significantly influenced, and over an extended period, in their prescribing patterns by industry practices such as free samples, free meals, industry-sponsored attendance at, and help with travel expenses to scientific conferences and participation in what is presented as a research presentation but is little more than a marketing exercise. Industry-sponsored symposia speakers, are more likely to prescribe the sponsor’s drug.
· Academic and research centers are also subject to industry’s influence, not only financially, e.g. funding of studies, but also in an indirect manner, through peer pressure, academic promotion etc. Government and the public have, hitherto, allowed the profession to practice self –regulation concerning these influences. However, demands from these sources for greater accountability are steadily growing in many countries.
IV. Specific concerns for professional bodies, training programs, researchers and clinicians.
· Advocacy for a complete severance of psychiatry’s relationship with industry is impractical. Prescribers must learn about available pharmacological options that will enable them to make informed choices. Failure to take the opportunity to gain new knowledge in this way, may deprive patients of treatments that could benefit them considerably. This could well be tantamount to providing negligent care.
· At the organizational and research levels, it is difficult to envision alternative sources of support for many activities that are essential to further the understanding of mental illness and its treatment. Many professional journals could not survive without industry or other external support. Governmental and non-industry sources of support are less likely to be made available for clinically-based research.
· Planning quality scientific conferences on the basis of participants’ registration fees alone is difficult to imagine. Additional sources of support, such as from the State, are unlikely, particularly in countries which are struggling just to provide basic services.
V. Suggestions
· Training programs should encompass a specific module to cover the ethical issues that arise in psychiatry’s relationship with industry.
· Trainee and qualified psychiatrists should keep abreast of scientific knowledge concerning the potential influences of industry on prescribing practices.
· Academic and consultant psychiatrists should be sensitized to the influence of role modeling on trainees as it relates to links with industry.
· Psychiatric services and especially academic centers should develop clear ethical guidelines regarding psychiatrists’ links with industry, including monitoring and auditing of joint activities.
· The industry should be encouraged to make unrestricted educational grants, so allowing recipients total freedom over choice of speakers and topics.
· Financial support from the industry should be given to institutions, such as psychiatric associations, university departments and research centers, rather than individuals,
in the form of unrestricted grants. These institutions
should be responsible for the allocation of the
funds in a transparent way.
· Free meals, gifts and services to individual psychiatrists should be eliminated
· Organizations should maintain a policy requiring industry- sponsored educational activities to be vetted for balance and objectivity by an authorised scientific program committee, as is the case with any other component of the program.
· The psychiatric profession should campaign against patient-direct advertising and assist relevant governmental departments to adopt corresponding policies.
This Draft was prepared by the WPA Standing Committee on Ethics.
Prof. Werner Pankratz prepared the original draft, Professors George Christodoulou and Sidney Bloch edited it and the members of the Committee reviewed it and contributed to the subsequent drafts.
Submitted on 15 August 2008 on behalf of the WPA Standing Committee on Ethics.
Prof. George Christodoulou
Chair, WPA Standing Committee on Ethics
MENU